Most Common Mistakes In Corrective Exercise
2024-06-12

Corrective exercise often gets a bad name, sometimes there are fair criticisms, but largely it is misunderstandings about the use and purpose of corrective exercise. Trust me, when you have been in an industry for almost 30 years as I have, you have made some of those mistakes so posts like this aren’t designed to judge people, but to help them not make the same mistakes.
In my experience, the issues with corrective exercise usually come down to three primary issues….
It Typically Isn’t ONE Thing!
Admittedly, I used to fall into this trap as a young coach. I would go to a course, it sounded awesome, made a lot of sense, it HAD to be the answer to all the corrective exercise issues my clients needed. That week I would be all excited to go “fix” everyone with all the new drills and information that I learned. By mid-week, I would be sitting in utter defeat once more.
How could I NOT be getting the results that the people who taught the course said were so possible to achieve? What was I doing so wrong? This often led me to going back and taking MORE courses with such groups and to be honest, this is very reasonable. I didn’t want to write off something because maybe I was making a mistake, maybe I was missing something, after all, I did JUST learn these techniques.
After a bit more time and taking more courses I would often be able to help some people here and there, but often not to the degree of fixing all the problems that my clients had. As a more mature coach I have a VERY different perspective upon this situation. First, there is no ONE fix for everyone. I don’t mean not just one drill, but no one method that will universally work for everyone because people are complex.
It isn’t just what we need physically that impacts our outcomes, but our attitudes and beliefs that influence things greatly as well. We have all heard of placebo and we think it is almost like something isn’t real. Actually, research shows that placebo is very powerful and should be harnessed more. One way to look at it is that when we BELIEVE something is likely to be helpful and positive to our goals, there is an increased chance that they will work. With the lesser known, nocebo, the opposite is true as well. So, you may have one client that thinks something is a the best idea ever and another may think it is nonsense. The one that believes it is the best idea is actually far more likely to have the same technique, exercise, method work than the one that doesn’t.

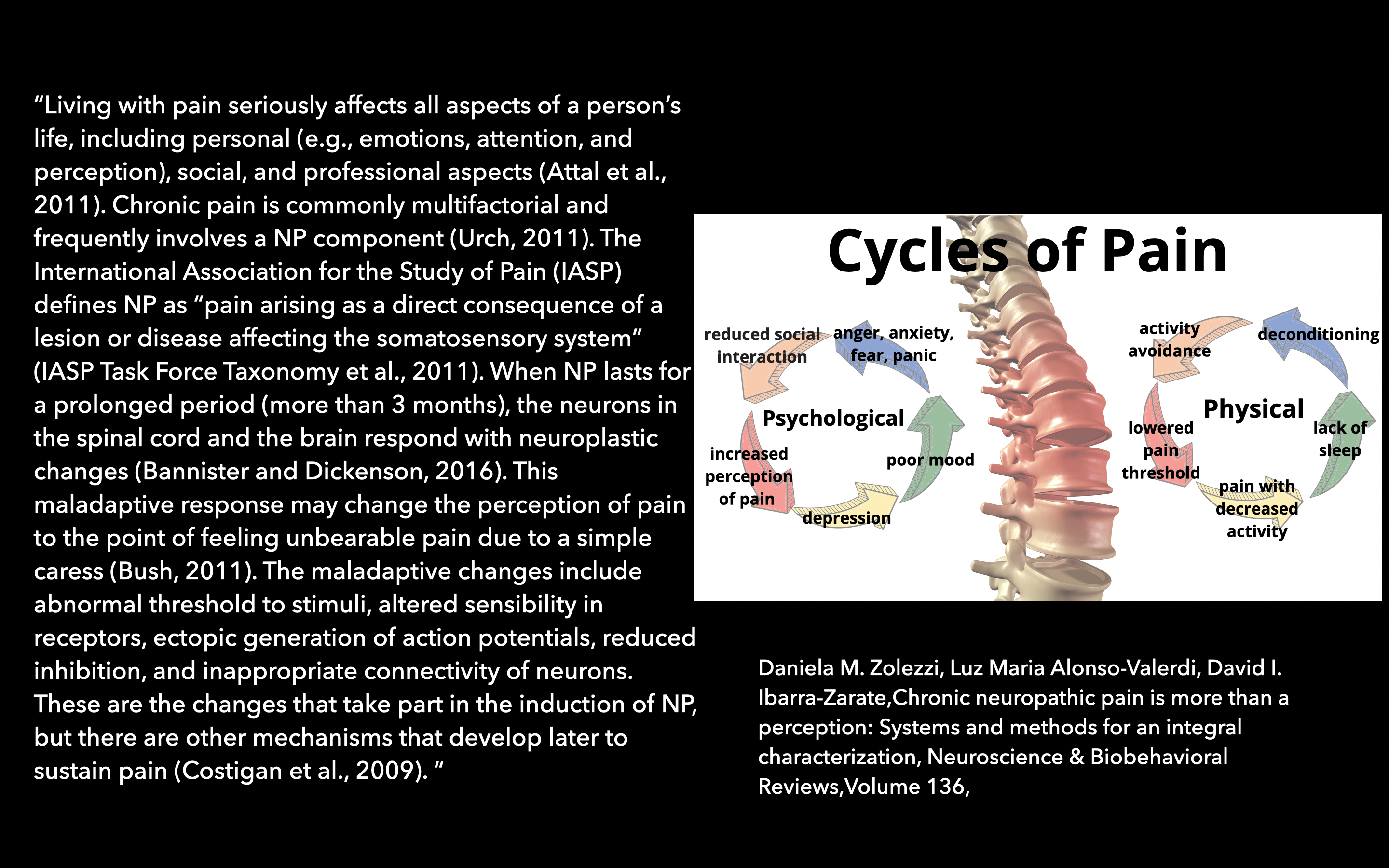
We are more complex than we are often taught to believe. That also means that issues we have can also be more complex. By complex I mean more multi-factorial. You could have some shoulder discomfort because you have a slight tear somewhere, you could ALSO have a bit of a neck issue causing some problems, you could also be really worrying about the shoulder issue that is making pain worse, you could also be having some life distress, not sleeping great, and so forth and so forth and so forth.
That doesn’t mean we try to address everything at once. The first step is to educate people on how pain works (something we should have at least a baseline understanding about or refer people to reliable resources) as just by educating people more, their pain levels can decrease.

My point is take in courses that discuss different ideas around corrective exercise, but never think that what you are learning is going to solve ALL the issues for your clients. Not all corrective exercise strategies (no matter how effective they are shown in research) are going to be attractive to all people either.
Individuals have a lot more control over their health and recovery than the best strength coach, fitness pro, and therapist do. So, we need to find things that can empower people to make incremental changes to their lifestyle that can cover a lot of bases at once.
Education is key, but so is making small changes to sleep and nutrition. These are VERY difficult things to change because they are behavioral and influenced by SO many emotional, attitude, and habitual actions. My best recommendation is to find 1-2 things that a person agrees is doable and they can work on being consistent. Remove the idea they will be perfect and just try for the first few weeks to be aware of these 1-2 action steps and see how they feel trying to implement them.
We HAVE to get people off the idea that they will do something once or twice and all their problems will be solved and they will be perfect from then on. It isn’t fair that pain, dysfunction, and so forth can feel like they came on suddenly and the fix will take some time. Setting forth proper expectations is key too!
People can perform, screen, and feel VERY different if their sleep and nutrition is improved (not fixed or perfect, but improved). That is why incremental and agreed upon strategies are key. Thrusting 30 action steps upon people make people feel overwhelming and almost inevitably sets them up to fail.
Not Looking & Looking Too Much For Issues
Both sides of the coin kinda work here. There are a lot of even fitness pros that ask me how to improve this or that quality with corrective exercise, when I ask them how they even measured that they need improvement, they often tell me they haven’t. Sadly too, sometimes the answer is because they can’t do some extreme exercise they saw on social media therefore they are “deficient” in mobility, stability, or strength. If you don’t even have any sort of measurement, you need a quantifiable one (subjective one’s are traps) and you need to make sure they fall in the realm of being reasonable and not some “feat” you want to achieve just because. There are many factors including your physical build, background, so forth and so forth that may determine if such feats of this or that are possible.
However, if you want to improve your shoulder mobility, for example, have some form of measurement. Not just moving your arms in flexion, but in all ranges of motion, also look at screening how areas that influence your shoulder mobility, such as neck mobility, core stability, and such are functioning as well. Remember, I don’t care what you use to determine this quantifiable measure (at least right now I don’t) but I want you to have something you can compare your progress to over time.

A different issue comes about when you look for anything and everything to be an iue. When I first started in the industry, I had a good friend that was training a NFL player. He wanted to make sure everything was being addressed for this athlete that he took him to one of the most popular corrective exercise experts at the time. The coach put this football player through an 8 hour assessment, not joking! Afterwards, some of the information was relevant, but a lot seemed like he was looking for a problem to identify. For example, he was told that one nostril was bigger than the other and he should see an ENT, not exaggerating.
My point is that depending upon what lens we look at issues from and how much we look, we can probably find issues that we could justify need corrective exercise work. Some might be reasonable, but chances are a lot are just looking to find “things”. Whenever I screen or am asked about screening for corrective exercise, there are a few keys I tell everyone.
The first is that your screening has to impact your programming. If your program gives everyone core stability exercises, for example, and the screen doesn’t give you insights on where to start with their core stability training, then it doesn’t make a lot of sense to do. Screening sometimes though can be just as helpful as to tell you what someone should NOT do as well. If someone shows consistently poor shoulder mobility, having them do a lot of overhead work doesn’t make a lot of sense. So, the screening has to help you know where to begin and what you will focus on, what not to do with someone, or don’t bother performing it.

Screening needs to be used in the framework of a system. If you have just a bunch of exercises (which most people honestly do) then it can be hard to figure out where to start with addressing some of these issues. That is why when people ask what corrective exercise we use in DVRT to address core stability, I tell them we just start at the beginning of our system. That is probably a dead bug press out with a heel drop, if that is too easy, we have strategies to make it just a bit more difficult. If it is too challenging, we have strategies to make is slightly easier. If you don’t have such methods for your corrective exercise, then you jump randomly from one exercise to another and that can be really frustrating for everyone involved.
There is A LOT more we could discuss, but I hope that makes people think a bit more how they are applying the concept of corrective exercise. I often find the issue is much less with the concept of corrective exercise and much more how it is begin framed and used by those that are trying to help improve how people feel, move, and perform.
If you want to learn more, don’t miss the great opportunity to save 40% on our DVRT Rx Shoulder Combo package that provides in-depth screens, education, and training ideas to help improve the wide array of factors that improve shoulder health and performance. Don’t miss it this week with code “combo” HERE
Featured in
© 2026 Ultimate Sandbag Training. Site by Jennifer Web Design.