Is the New Science Of Pain Bogus?!
2026-05-26

Recently, social media has started pushing back against brain reprocessing techniques for chronic pain. Some posts argue there’s “little evidence,” while others claim these approaches are basically telling people that “pain is all in your head.”
Like most social media debates, the truth is more nuanced.
The problem isn’t that pain neuroscience, somatic tracking, or brain reprocessing concepts are completely wrong. The problem is that these ideas are often poorly explained, oversimplified, or presented in an extreme way that ignores the complexity of pain itself.
At the same time, some critics swing too far in the opposite direction and act as though the brain plays little role in chronic pain.
Both perspectives miss the mark.
Chronic Pain Is Real And the Brain Is Involved
One of the most important findings in pain science over the last two decades is that chronic pain is not simply about tissue damage.
A well-known Northwestern University study helped demonstrate that people transitioning from acute pain to chronic pain showed changes in neural network activity in the brain. In other words, persistent pain is associated with measurable changes in how the nervous system processes information.
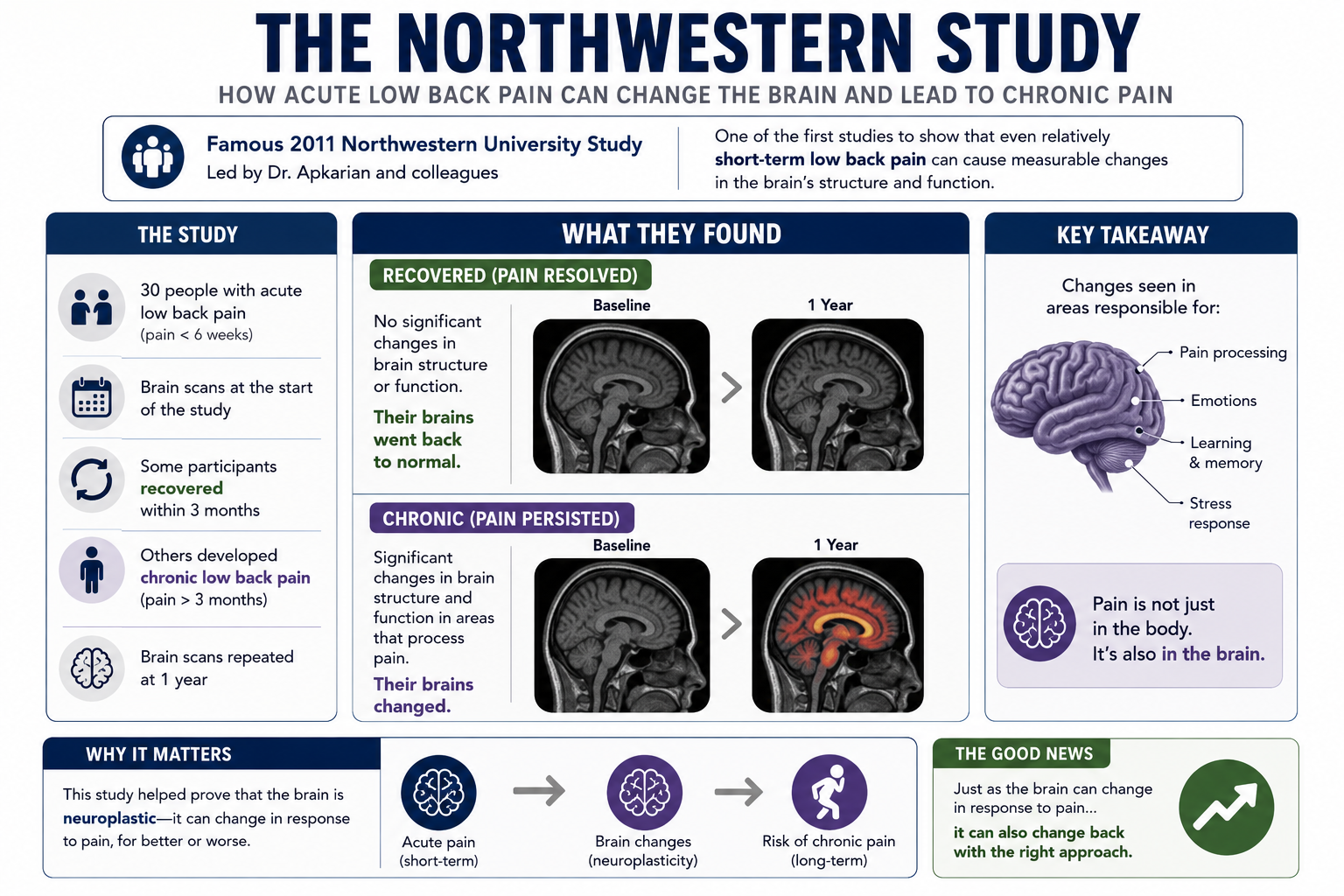
This does NOT mean pain is imaginary.
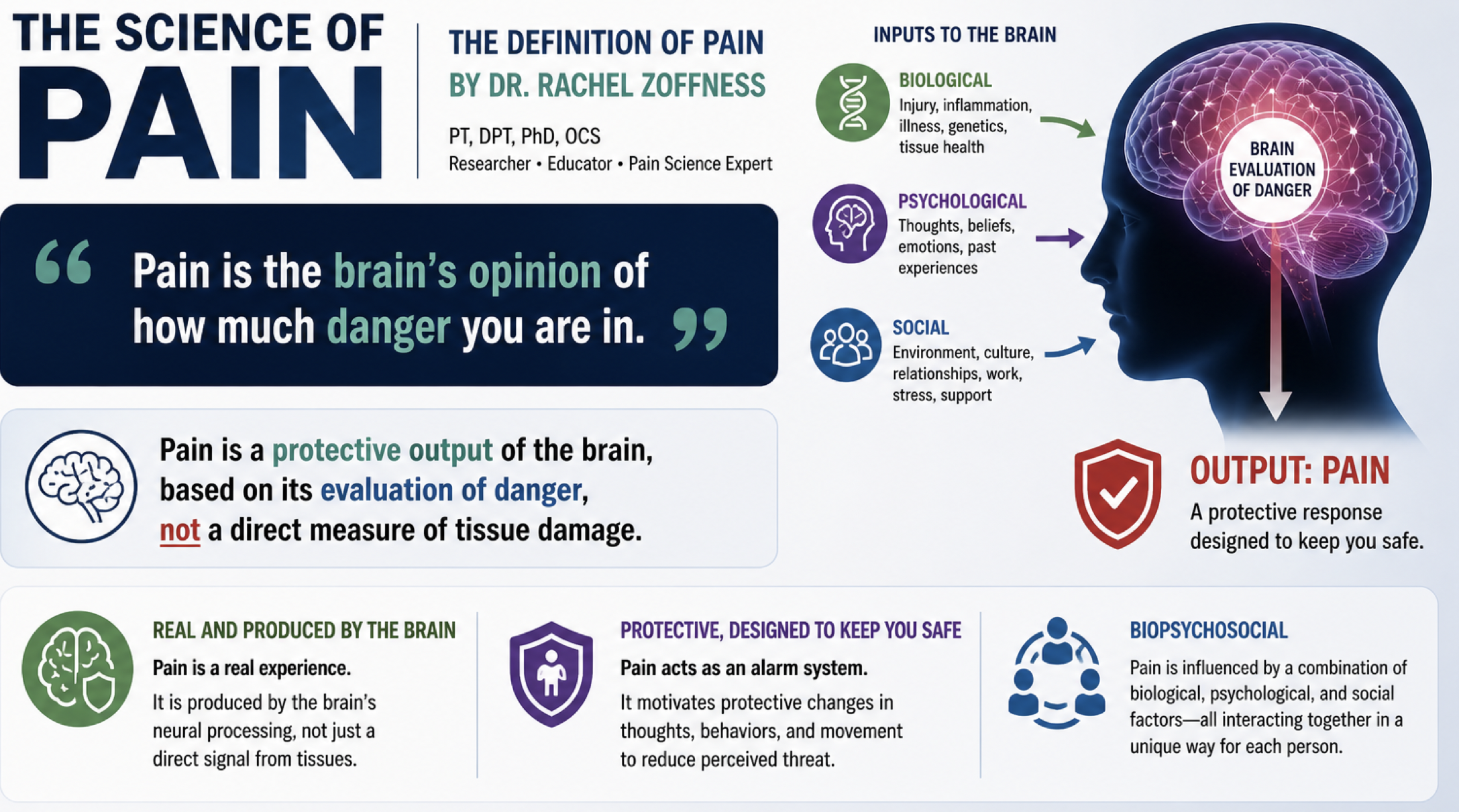
It means the experience of pain is influenced by the nervous system’s interpretation of threat, safety, attention, stress, memory, emotions, and past experiences.
Pain is always real. But pain is also an output of the brain.
That concept makes many people uncomfortable because they assume it means:
“The pain isn’t physical.”
But that’s not what pain science is saying.
The False Divide Between “Physical” and “Psychological”
One of the biggest mistakes happening online is the creation of a false choice:
Either:
pain is structural and physical,
or:
pain is brain-generated and psychological.
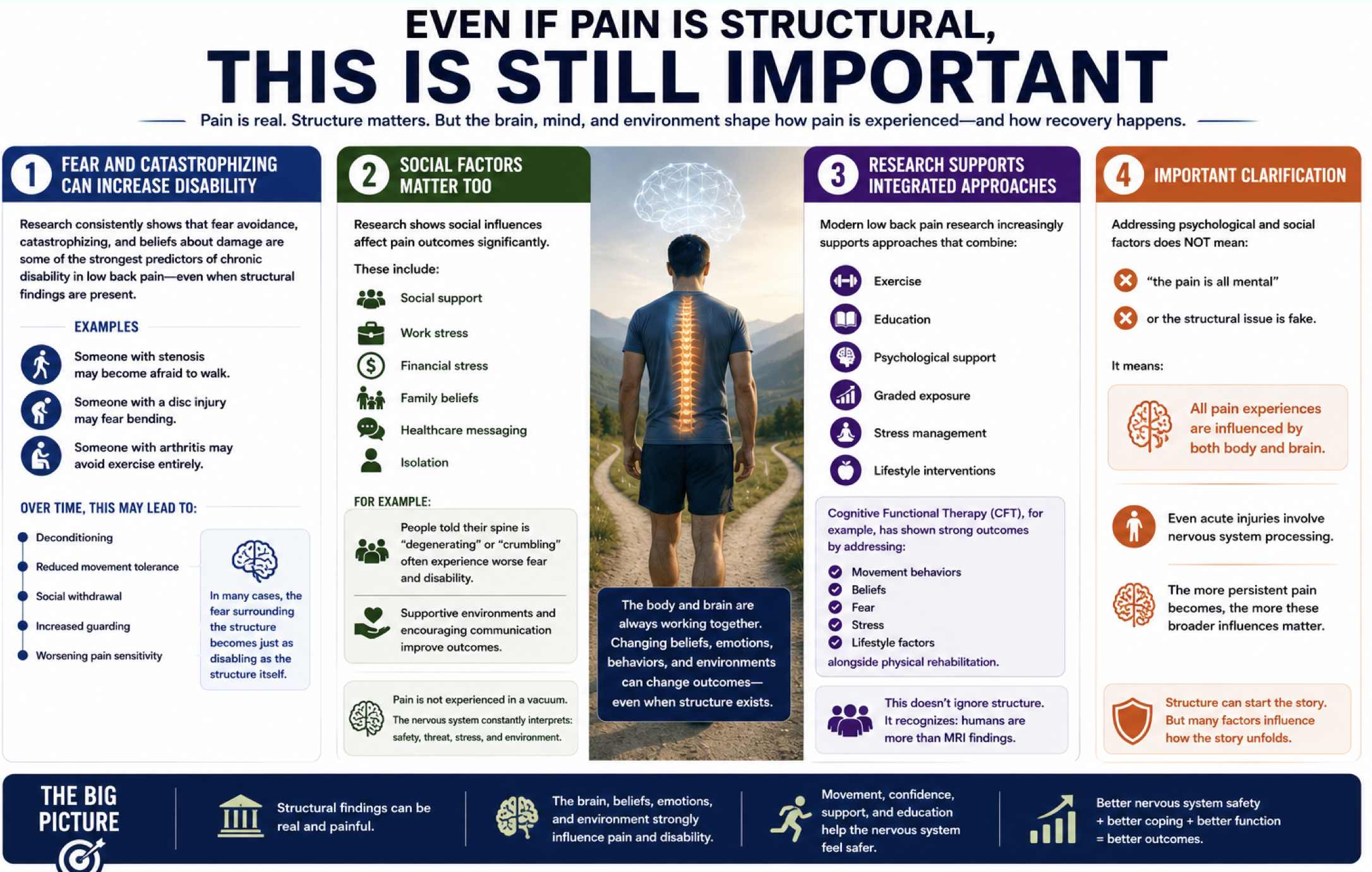
In reality, chronic pain is usually both biological and neurological, while also being influenced by psychological and social factors.
This is the biopsychosocial model, not as a trendy buzzword, but as a practical reality.

Physical qualities still matter tremendously.
Strength matters.
Mobility matters.
Endurance matters.
Sleep matters.
Movement variability matters.
Load tolerance matters.
If someone has poor conditioning, movement fear, deconditioning, weakness, poor recovery, high stress, and reduced confidence in movement, all of those factors can influence pain.
The brain and body are not separate systems competing for attention. They are deeply connected.
Exercise Is One of the Most Powerful Pain Interventions We Have
Ironically, some debates online frame pain neuroscience and exercise as opposing ideas.
The research says otherwise.
Exercise consistently shows benefits for chronic pain across:
biological health, psychological health, and social well-being.
Movement can improve:
- strength,
- circulation,
- tissue capacity,
- nervous system regulation,
- mood,
- confidence,
- stress resilience,
- and overall quality of life.
Exercise is one of the few interventions that positively impacts almost every aspect of human health simultaneously.
But here’s where things become interesting.
The way we approach exercise matters.
Trying to “Fix” Pain Often Backfires
Many people exercise with one goal:
“I need to get rid of this pain.”
That sounds logical, but it can create a problem.
When every workout becomes a test:
“Did my pain go away?”
“Did this fix me?”
“Am I damaged?”
“Why do I still hurt?”
…the nervous system can stay hyperfocused on symptoms.
Pain becomes the center of attention.
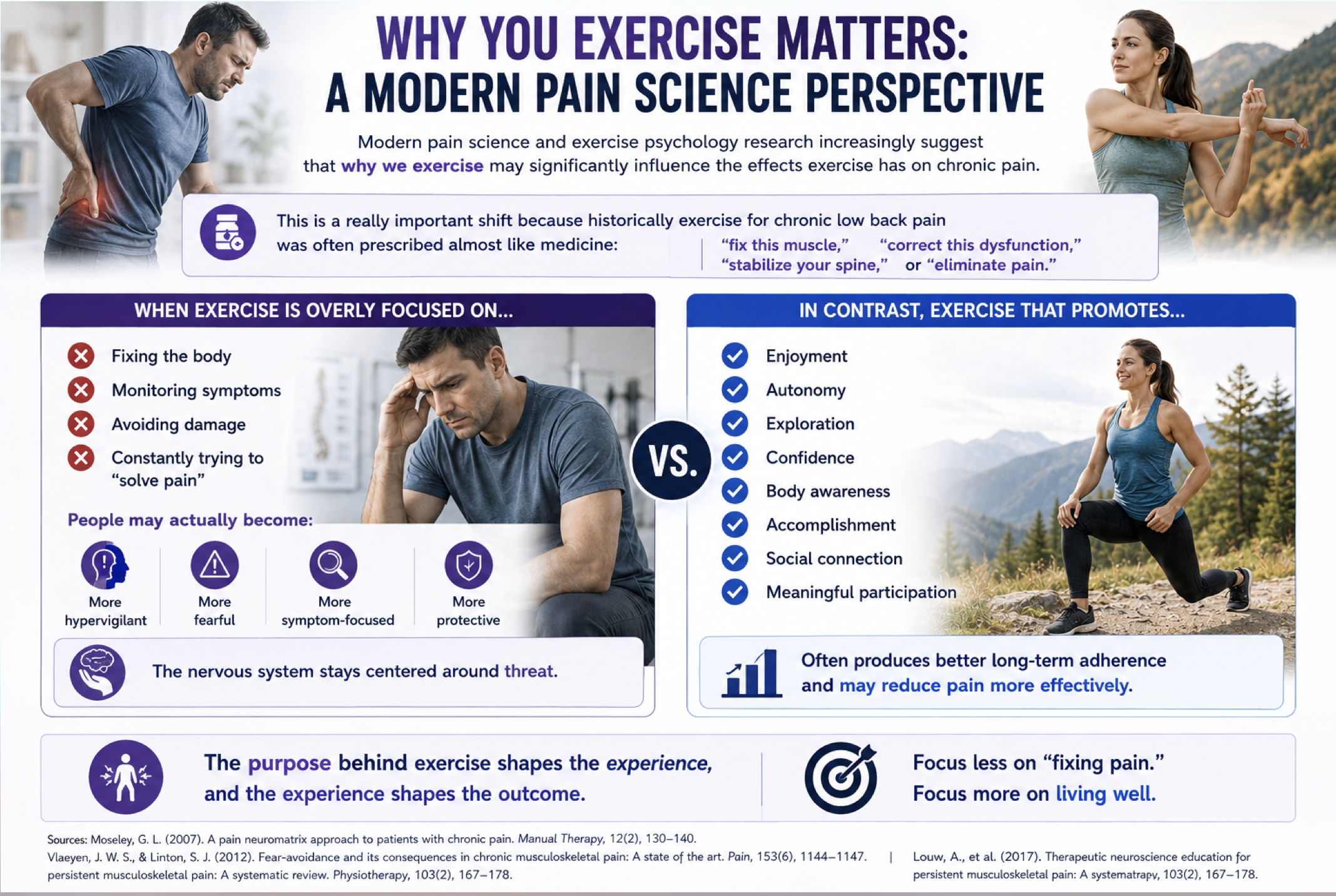
Ironically, this can reinforce fear, frustration, hypervigilance, and protective tension.
Research and clinical experience increasingly suggest that people often do better when movement becomes less about chasing pain relief and more about:
- building confidence,
- improving capability,
- enjoying movement,
- reconnecting with their body,
- and feeling safe during activity.
That shift matters.
Confidence Changes the Experience of Pain
One of the most overlooked qualities in rehabilitation is movement confidence.
When people begin to trust: their body, their movement, and their ability to adapt, their nervous system often becomes less reactive.
This doesn’t mean pain instantly disappears.
But the relationship to pain changes.
Instead of:
“Something must be wrong.”
The mindset gradually becomes:
“My body is adaptable, resilient, and capable.”
That psychological shift can influence physiology more than many people realize.
- Fear changes muscle tension.
- Fear changes breathing.
- Fear changes attention.
- Fear changes movement patterns.
- Fear changes stress chemistry.
Confidence can change those things too.
Brain Reprocessing Is Probably Neither a Miracle Nor a Scam
This is where the online conversation tends to become unhelpful.
Some people promote brain reprocessing as though every chronic pain condition is entirely generated by the brain and can be solved through mindset work alone.
That’s clearly an oversimplification.
At the same time, dismissing nervous system retraining entirely ignores a growing body of evidence showing that: fear, attention, catastrophizing, stress, emotional regulation, and learned pain responses all influence pain sensitivity.
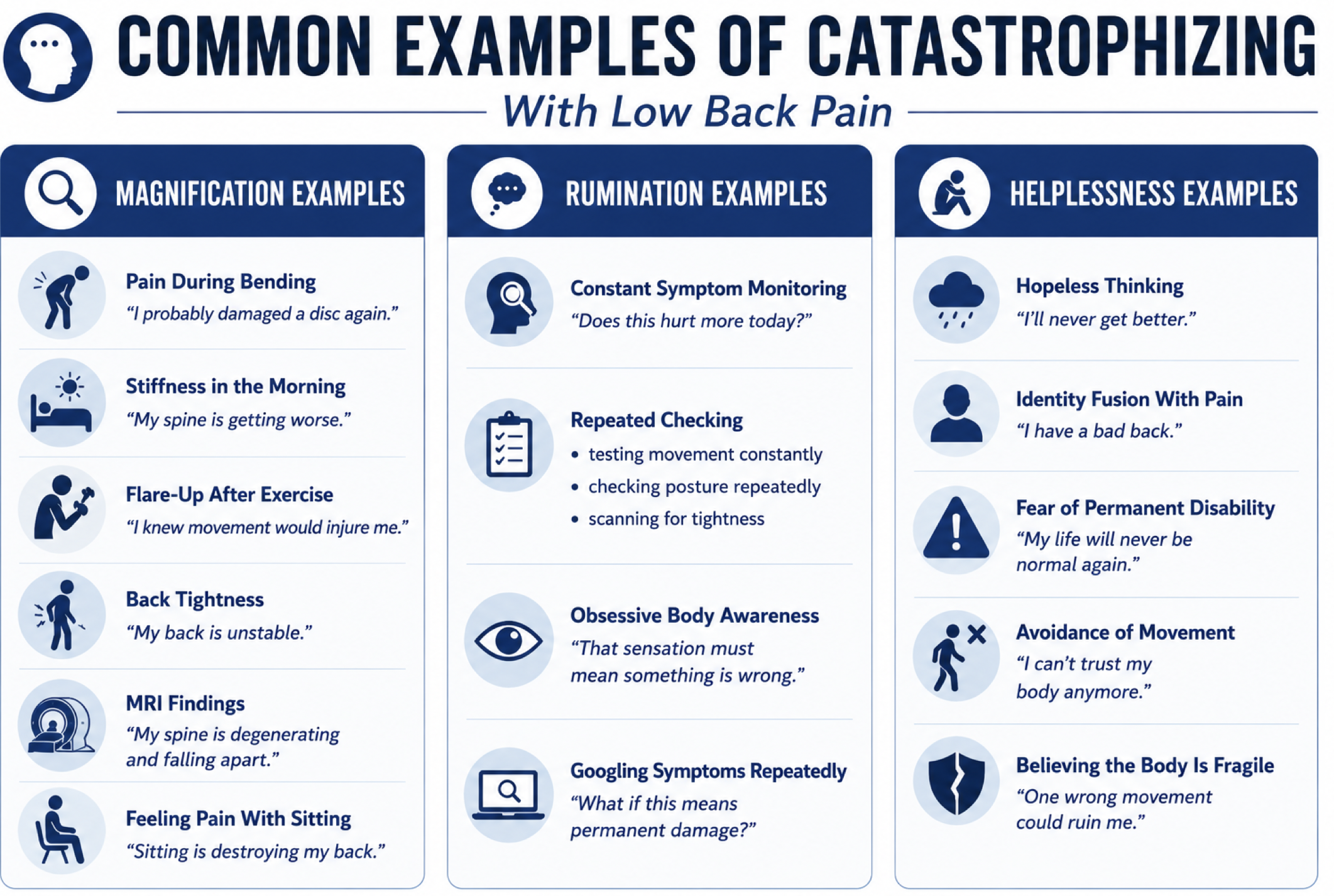
The nervous system can absolutely become more protective over time.
But improving chronic pain usually requires addressing multiple layers:
physical capacity, movement confidence, stress regulation, sleep, recovery, beliefs, emotions,
and lifestyle habits.
No single intervention explains everything.
The Better Goal
Maybe the better goal isn’t obsessing over whether pain is “structural” or “brain-based.”
Maybe the better question is:
“What helps people move, feel, and live better?”
For many people, that includes: strength training, graded exposure, aerobic exercise, better recovery, mindfulness, somatic tracking, improved sleep, stress management, and rebuilding trust in movement (not all at once obviously and maybe not all of it).
Not because pain is fake.
But because humans are complex.
And the more we stop reducing chronic pain to simplistic social media arguments, the more effectively we can help people move forward.
Find out a better way to interpret the science of low back pain at our NEW and upcoming Low Back Pain Masterclass. For the rest of this week you can save 20% with code “back20” HERE
Featured in
© 2026 Ultimate Sandbag Training. Site by Jennifer Web Design.